News
Biden seeks to ramp up money to beat HIV/AIDS in budget request
$267 million increase sought to end domestic epidemic

President Biden’s formal budget proposal for the U.S. government in the upcoming fiscal year has advocates in the fight against HIV/AIDS cheering over the commitment to increase funds to confront the domestic epidemic, although one group is criticizing the proposal for seeking to flat-fund international programs.
The fiscal year 2022 proposal, unveiled last Friday, would afford an additional $246 million for domestic HIV testing, prevention and treatment programs for the Ending the HIV Epidemic initiative, which seeks to end HIV by 2030, and would also provide a general boost of $46 million to Ryan White HIV/AIDS programs and $20 million for HUD’s Housing Opportunities for People with AIDS (HOPWA).
Carl Schmid, executive director of the HIV + Hepatitis Policy Institute, said in a statement Biden is “demonstrating his commitment to ending HIV in the United States” in the budget request to Congress.
“While it falls short of what is needed and the community has requested, if this funding is realized it will continue the momentum already created and make further progress in ending HIV in the U.S. Efforts to end HIV will help eradicate an infectious disease that we have been battling for the last 40 years and help correct racial and health inequities in our nation,” Schmid said.
The total $670 million requested by the White House for the Ending the HIV Epidemic initiative breaks down as follows:
- Centers for Disease Control & Prevention: $100 million in new money for a total of $275 million;
- Ryan White: $85 million in new money for a total of $190 million;
- Community Health Centers for PrEP: $50 million in new money for a total of $152 million;
- National Institues of Health: $10 million in new money for a total of $26 million;
- Indian Health Services: $22 million in new money for a total of $27 million.
Counterinituitively, each of those numbers is actually below what the Trump White House proposed in the previous administration’s final budget request, with the exception of the proposed increase in money for Community Health Centers for PrEP and flat-lining for money for Indian Health Services.
The requested increase in funds for the Ending the HIV Epidemic was expected. Biden had signaled he’d seek the additional $267 million in funding in the “skinny budget” issued by the White House in February that preceded the more formal and detailed request to Congress last week.
Biden requests the increase in funds after he campaigned on ending the domestic HIV epidemic by 2025, an ambitious goal many advocates in the fight against HIV/AIDS were skeptical about achieving.
Nick Armstrong, the AIDS Institute’s manager of advocacy and government affairs and co-chair of the AIDS Budget & Appropriations Coalition, said in a statement the time to ramp up efforts against HIV has come as the nation emerges from the coronavirus pandemic.
“Public health departments have made herculean efforts to battle COVID over the past year,” Armstrong said. “But now it is time to reinvigorate neglected efforts to end the HIV, opioid, and viral hepatitis epidemics. Congress must go above and beyond what the president has proposed to bolster our critical public health infrastructure to protect Americans against infectious disease.”
The budget now goes on to Congress, which has authority on whether or not to appropriate funds consistent with the president’s request. Congress could either meet, short fund or even exceed in money the request by Biden as part of that process.
Schmid said via email to the Blade he’s optimistic about getting an agreement from Congress for an increase in funds to fight HIV/AIDS based on the “strong bipartisan support the proposal has enjoyed in the past.
“We still have work to do with the Congress due to so many demands on the budget but I am fairly confident Congress will support it, they have been anxious to see what the Biden administration does with the program in his budget and we have the answers now,” Schmid said. “The Biden-Harris administration firmly supports ending HIV.”
Although Biden was lauded for the increase in funds in domestic HIV programs, international programs are a different matter. The White House has essentially flat-funded programs designed to fight the global HIV epidemic, including the President’s Emergency Plan for AIDS Relief, or PEPFAR, or the Global Fund to Fight AIDS, Tuberculosis & Malaria.
Matthew Rose, director of U.S. Policy and Advocacy at the New York-based Health GAP, said in a statement Biden’s budget proposal “displays a lack of bold leadership motivated to end the HIV pandemic.”
“If the U.S. had continued fully funding PEPFAR since 2003 instead of letting funding levels slip into a flat-line for more than a decade, the HIV pandemic would look remarkably different today,” Rose said. “This is not a budget to end AIDS – and it could have been. This is not a budget to end the COVID-19 pandemic – and it could have been. The unconscionable lack of political will in recent years has created a world in which people cannot get access to the life-saving services they need.”
Health GAP is calling on Congress to approve a budget with at least a $750 million increase for PEPFAR and $2.5 billion in increased funding over the next four years to scale up HIV prevention and treatment and mitigate harms to the HIV response done by the COVID-19 pandemic, the statement says.
Additionally, Health GAP is calling on Biden to name “a highly qualified nominee” to serve as the U.S. Global AIDS Coordinator, the statement says.
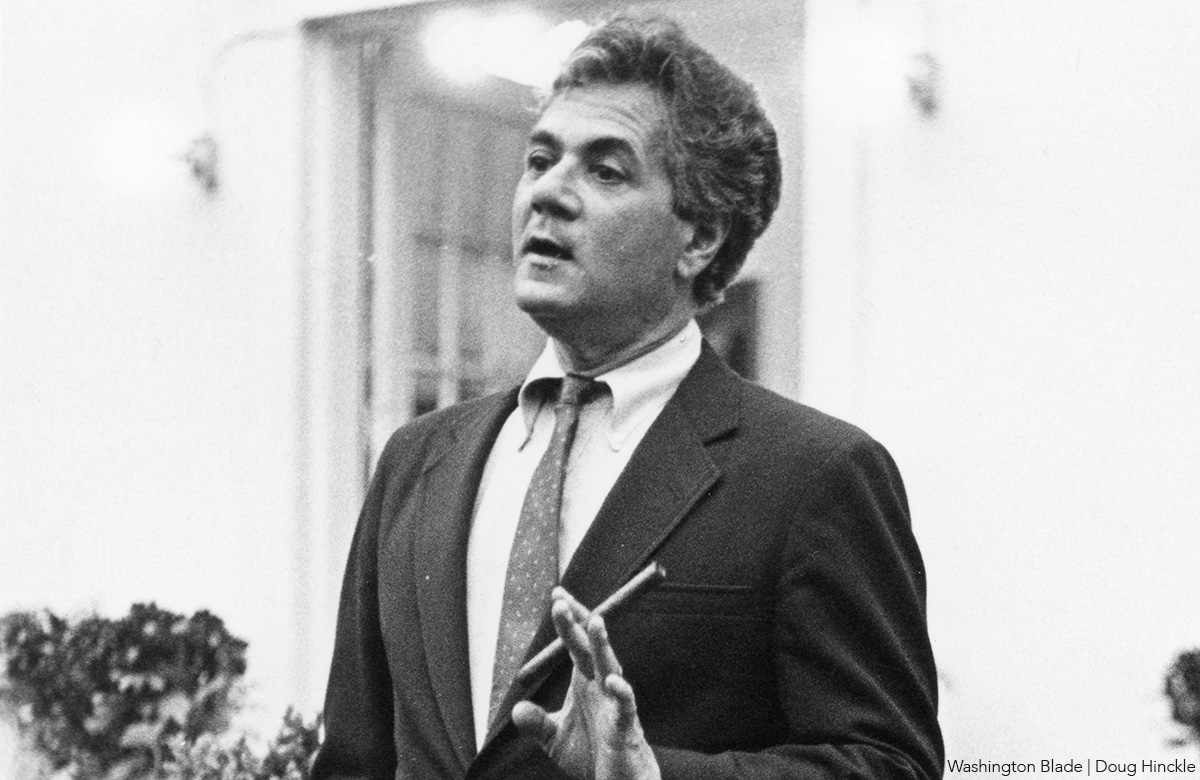
Former U.S. Rep. Barney Frank (D-Mass.), who served in the U.S. House of Representatives from 1981 until his retirement in 2013 and who became the first member of Congress to voluntarily come out as gay in 1987, died on May 19, at the age of 86, at his home in Ogunquit, Maine.
His passing came less than a month after he announced he had entered home hospice care due to terminal congestive heart failure under the care of his husband, Jim Ready, and shortly after finishing writing a new book entitled, “The Hard Path to Unity: Why We Must Reform the Left to Rescue Democracy.”
Despite his frail health, during the last few weeks of his life, Frank agreed to do interviews with multiple news media outlets, including the Washington Blade, where he reflected on his sometimes-controversial positions on issues such as transgender rights.
He told the Blade he had been living with his husband in their shared home in Maine since the time of his retirement in 2013 and called his husband a “saint” for caring for him during his illness. In 2012, at the age of 72, Frank married Ready, becoming the first sitting member of Congress to marry someone of the same sex.

News of his passing prompted an outpouring of praise and reflection on his life as a groundbreaking out gay lawmaker by current and former members of Congress and LGBTQ rights leaders.
Massachusetts Gov. Maura Healey announced on May 20 that she had ordered the U.S. flag and the state flag to be lowered to half-staff at all state buildings in honor of Frank’s life and legacy and the recognition of his passing.
“Barney Frank was nothing short of a trailblazer,” said Kelley Robinson, president of the Human Rights Campaign, the nation’s largest LGBTQ advocacy organization, in a statement. “At a time when being openly gay in public service could cost you everything, he chose visibility,” Robinson said.
Robinson and other LGBTQ advocates also pointed to Frank’s role in speaking out in Congress for stronger efforts to address the AIDS epidemic during the early years of HIV/AIDS, his push for the repeal of the “Don’t Ask, Don’t Tell” policy to initially allow gays to serve openly in the military, the enactment of marriage equality for same-sex couples, and broader anti-discrimination protections.
Frank has also been credited with helping to pass the federal Matthew Shepard and James Byrd Jr. Hate Crimes Protection Act of 2009.
In addition to his longstanding support for LGBTQ rights, political observers have said one of his most important achievements in Congress was his role, as chair of the House Financial Services Committee, in becoming co-author of what became known as the Dodd-Frank Wall Street Reform and Consumer Protection Act of 2010.
Coming at the time of a nationwide banking crisis, the New York Times has called the Frank bill that he and then-U.S. Sen. Christopher Dodd (D-Conn.) wrote “the most significant overhaul of the nation’s financial regulations since the Great Depression.”
Frank was born and raised in Bayonne, N.J., and graduated from Bayonne High School.
He graduated from Harvard College in Massachusetts in 1962 and worked in various places, including as an assistant to then-Boston Mayor Kevin White, before winning election to the Massachusetts House of Representatives in 1972, where he served for eight years representing a Boston area district. During that time he attended and graduated from Harvard Law School and became a member of the Massachusetts bar in 1979 after passing the bar exam.
In 1980, Frank became a candidate for the U.S. House in the Massachusetts 4th Congressional District, which he won with 52 percent of the vote in a four-candidate race, taking office in January 1981. He won re-election decisively over the next 30 years until announcing in 2012 his plans to retire and he would not run for re-election that year.
The New York Times is among the publications that have reported this week since Frank’s passing that his record as an esteemed and admired lawmaker helped him survive a sex scandal that surfaced in 1990 linking him to male prostitute Stephen Gobie.
Media reports at the time said Frank had patronized Gobie as one of his customers and for a time had Gobie as a roommate in Frank’s D.C. residence in the Capitol Hill neighborhood. In its article this week, the New York Times says Gobie “claimed that in the mid-1980s he had run a prostitution ring out of Mr. Frank’s home.”
Like other media accounts, the Times report adds that following an investigation, “The House Ethics Committee did not substantiate that claim, but it did find that Mr. Frank had fixed 33 parking tickets for Mr. Gobie and sought to shorten his probation on drug and sex-offense convictions by writing a misleading memorandum on congressional stationery to an official involved in supervising Mr. Gobie’s probation.”
The full House voted 408-18 to reprimand Frank for misuse of his office, but it rejected calls by some to censure or expel him.
“I should have known better,” Frank said in a speech on the House floor at that time, according to the New York Times. “There was in my life a central element of dishonesty,” the Times quoted him as saying. “Three years ago, I decided concealment wouldn’t work. I wish I decided that long ago,” he said referring to his 1987 decision to come out publicly as gay.
Despite all of this, Frank was re-elected that year with 66 percent of the vote, a development that his friends and supporters attribute to his reputation as a beloved and highly regarded public figure.
PFLAG, the national advocacy group for parents and friends of LGBTQ people, is among the groups that issued statements this week reflecting on Frank’s positive impact on the LGBTQ community.
“Frank was not only the first openly gay member of Congress, but he was also co-author of the Dodd-Frank Wall Street Reform and Consumer Protection Act of 2010 as chair of the House Financial Services Committee, which helped enshrine housing access for LGBTQ+ people,” PFLAG says in a statement.
“He was also a leading advocate on laws to combat HIV/AIDS,” the statement says, adding that PFLAG’s national office honored Frank with its Champion of Justice Award in 2018.
“Barney was candid, outspoken, quick-witted and downright funny, and he always had his eye on making progress,” said U.S. Sen. Tammy Baldwin (D-Wis.), the first openly lesbian woman elected to the U.S. Senate, in a statement. “He was willing to take on anyone who was in his way, regardless of who they were — I should know, I was one of the many who on occasion got an earful from him,” Baldwin said.
‘But I, and anyone else who spent time with him, were lucky to watch him in action and learn from him,” her statement continues. “Barney was a masterful legislator, savvy and strategic, and always thinking of the long game,” she said. “Our country is a better, more just, more equal place because of him, and he will be sorely missed.”

U.S. Rep. Mark Takano (D-Calif.), who serves as chair of the Congressional Equality Caucus, which represents LGBTQ members of Congress and their congressional allies, issued his own statement on behalf of the caucus pointing out that Frank was one of the two founding members of the caucus.
“I was honored that he came to campaign for me during my run for Congress just a few years after he co-founded the Congressional Equality Caucus, which I now have the distinct honor of leading,” Takano said.
He was referring to Frank and then-Congresswoman Tammy Baldwin’s action in 2008 to found the House LGBT Equality Caucus as the only two openly gay members of Congress, which evolved into the Congressional Equality Caucus.
“Barney proved that what mattered most was the work you did for others,” Takano says in his statement. “I truly believe that we are closer to a more equal world because of Barney Frank,” he said, adding, “Congressman Frank’s legacy touches every part of our fight for LGBTQI+ equality: from his work advocating for HIV and AIDS research to helping pass major pro-equality legislation like the Don’t Ask, Don’t Tell Repeal Act and the Hate Crimes Prevention Act into law.”
In his May 5 interview with the Blade, Frank responded to criticism he received during his tenure in Congress from some LGBTQ rights advocates, especially trans activists, who claimed he had not provided sufficient support for trans rights legislation.
He said he fully supported ongoing efforts to advance trans rights but said those efforts could be jeopardized by pushing issues for which many voters have yet to accept, such as “male to female transgender people playing in women’s sports.”
Among those praising Frank’s life and legacy at the time of his passing is longtime trans activist Diego Sanchez, who became the first openly trans congressional staffer when Frank hired Sanchez as his office’s Senior Policy Advisor. Sanchez remained on Frank’s staff until Frank’s retirement in 2013.
“Barney was a revered statesman for our country at the local, state, and federal levels and a treasured friend to me,” Sanchez told the Blade in a statement. “His belief that prejudice comes from ignorance and is only stricken by visibility explains how he came out openly and how he brought me to his staff, with intent and without apology,” Sanchez said.
He added, “I miss him terribly and am glad I got to spend a week with his husband Jim and him this month. Barney made sure that members of Congress could not say they had never met a trans person. I was honored to be a groomsman in their wedding and will miss Barney’s brilliance, counsel, friendship, and wit.”
Sanchez said celebration of life events are expected to take place in Boston and D.C. and details of those events will be announced soon.
India
Iran war causes condom shortage in India
Trade disruptions have strained petrochemicals, lubricant supplies

About 80 days into the U.S.-Iran war, while much of the world struggles with oil supplies, India is confronting a different crisis: a widening condom shortage. Health activists warn the supply disruption could worsen HIV/AIDS risks in the world’s most populous country.
Disruptions in maritime trade through the Strait of Hormuz have strained supplies of petrochemicals and industrial lubricants used in condom manufacturing. The crisis has increased production costs across the sector and pushed retail prices sharply higher.
India’s condom manufacturing industry is valued at nearly $1 billion.
Production depends heavily on silicone oil and ammonia. Silicone oil, a key lubricant used in manufacturing, is in short supply. Ammonia, which stabilizes raw latex, is expected to see price increases of 40-50 percent. Rising packaging costs have added further pressure. Some manufacturers and retailers have reported condom prices increasing by as much as 50 percent.
India is home to an estimated 2.5 million people living with HIV, the world’s second-largest population of HIV-positive people, according to a 2024 report. The Health Ministry’s India HIV Estimation 2025 technical report said 5.4 percent of HIV cases in 2024-2025 were linked to transmission between men who have sex with men.
In 2024, India recorded an estimated 64,470 new HIV infections and 32,160 AIDS-related deaths nationwide. The figures marked declines of 48.69 percent and 81.42 percent, respectively, compared with 2010.
Ankit Bhuptani, an LGBTQ activist in India, told the Washington Blade that the country has made significant progress in reducing HIV infections over the past two decades. But, he said, that progress depended heavily on affordable condoms, targeted outreach programs and on-the-ground work by NGOs serving MSM and transgender people.
“Pull one thread and the whole thing loosens. What worries me about this particular shortage is that it arrives at exactly the moment when India’s LGBTQ community was beginning to access healthcare more openly after the Section 377 reading down,” said Bhuptani. “Young queer Indians in tier-two cities were just starting to trust government health systems enough to engage with them. A price spike that prices them out, or a shortage that sends them to substandard alternatives, could set that trust back by years.”
The Indian Supreme Court in 2018 struck down Section 377, a colonial-era law that criminalized consensual same-sex sexual relations.
In March, the Commerce and Industry Ministry acknowledged the difficulties faced by Indian exporters due to disruptions caused by the war in West Asia and launched a roughly $51.5 million Resilience and Logistics Intervention for Export Facilitation, or RELIEF, program. It provides credit insurance support for exporters whose shipments have been stranded because of the conflict.
“Price elasticity in sexual health products is brutal. When a condom pack goes from 20 rupees to 40, usage drops. It’s that simple,” said Bhuptani. “And when usage drops in populations with higher baseline HIV exposure, you don’t see the consequences for two or three years. Then the numbers arrive and everyone acts surprised.”
The situation has been further aggravated by the structure of India’s condom market, which operates on a high-volume, low-margin model designed to keep products affordable for a population of more than 1.4 billion people. Industry analysts say that model is now under growing pressure from rising raw material and shipping costs.
Reports in Indian media said supply constraints and price volatility involving PVC foil, aluminium foil, and packaging materials have disrupted production and complicated order fulfilment across parts of the condom manufacturing sector.
“Supply chain vulnerability assessments almost never include sexual health commodities. They should. India imports roughly 86 percent of its anhydrous ammonia from West Asian countries including Saudi Arabia, Qatar, and Oman, with that ammonia being essential for stabilizing the natural rubber latex used in domestic condom production,” said Bhuptani. “That is a documented strategic dependency that was never flagged as a risk. The Iran war converted it from a latent vulnerability into an active supply shock in a matter of weeks.”
The National AIDS Control Organization, or NACO, which oversees India’s HIV/AIDS programs, during the 2026-2027 fiscal year received an allocation of about $249 million, up from roughly $238 million the previous year. By comparison, the U.S. approved a $6 billion funding package in 2026 for global HIV/AIDS programs, according to the United Nations.
“The gay and trans community in India report high perceived HIV risk and adopted PrEP through non-profit and private channels, with cost and access remaining consistent concerns,” said Bhuptani. “The community organizations managing that risk perception are now operating in a tighter supply environment while simultaneously absorbing the downstream effects of USAID funding cuts. Health workers seeing increased anxiety among community members are observing the predictable consequence of removing redundancy from a system that had very little to begin with.”
The Washington Blade reached out to Indian condom manufacturer Manforce several times, but the company declined to comment.
Harish Iyer, an LGBTQ and equal rights activist in India, told the Blade that this is the time when the government needs to step in. Condoms, Iyer said, are not about pleasure, but about life.
“Not just in terms of HIV, it is also a source of contraception in a nation which is heavily populated. So, if there is a crisis in the condom industry, it has an adverse effect on the LGBTQ community,” said Iyer. “And eventually it has a compounding effect on the economy as well. Because if the cases of HIV wrecks to rise, if the population was to explode, it is going to have a straining effect on the economy as well. So, I think it is time that the government steps in, and condoms should be recorded as a necessity commodity rather than making it feel like any kind of commodity that some (privileged people) can afford.”
Iyer told the Blade that the government should provide condoms free of cost.
He pointed to the Nirodh Scheme, India’s long-running family planning and safe sex program launched by the government in 1968. Condoms, Iyer said, are a necessity, not a luxury product. He urged the government to classify them as essential items and either remove the Goods and Services Tax or reduce it to a minimum.
The Nirodh Scheme was launched by the Health and Family Welfare Ministry to promote contraception and prevent the spread of sexually transmitted infections, including HIV, through the nationwide distribution of subsidized and free condoms.
Wyoming
U.S. attorney nominee confirmed despite anti-LGBTQ history, no trial experience
Nine felony grand jury indictments tied to Darin Smith dismissed last week

Republicans confirmed Darin Smith as U.S. Attorney for the District of Wyoming on Monday, regardless of his history as interim U.S. Attorney for Wyoming and a state senator.
While serving as interim U.S. Attorney for Wyoming — after being appointed by President Donald Trump last July despite never trying a case outside of his time as a law student intern — former state Sen. Darin Smith likely prejudiced jurors during grand jury proceedings.
Nine felony grand jury indictments tied to Smith’s tenure were dismissed last week.
Judges dismissed felony indictments against Cheyenne Swett, Richard Allen, Michael Scott Hopper, Brian Joseph Johnson, Dennison Jay Antelope, Matthew Christopher Jacoby, Matthew Miller Jr., Wolf Elkins Duran, and Jose Benito Ocon. The now-dismissed charges included felony firearm possession, drug distribution, and possession of child pornography, among other allegations.
Smith allegedly told the grand jury that the defendants were “bad guys,” described them as “murderers,” and said deliberations “won’t take long.”
Even the U.S. Attorney’s Office for the District of Wyoming acknowledged that Smith’s comments were “ill-advised.”
Smith has a history of aligning with Trump over the Constitution and supporting anti-LGBTQ legislation.
In 2025, Smith co-sponsored House Bill 0194, titled “Obscenity amendments,” which, among other provisions, would have criminalized drag shows. The bill also would have repealed exemptions for public and school librarians from the crime of “promoting obscenity” to minors. The wording of the bill was so vague that Republican state Rep. Lee Filer said, “We will end up having to arrest somebody for allowing a child to read the Holy Bible.”
Smith also co-sponsored SF0062, a bill requiring public school students to use restrooms, sex-designated changing facilities, and sleeping quarters that align with their sex assigned at birth. In March 2025, the Wyoming governor signed the bill into law, along with its House companion.
He also attended the Jan. 6 Capitol riot alongside thousands of other Trump supporters.
“Smith was on the Capitol grounds on Jan. 6 … and made the reprehensible claim … that the hundreds of Capitol Police officers who risked their lives that day were guilty of ‘massive incompetence.’ Smith blames the police for what happened on Jan. 6. Without evidence, he claimed that rioters who breached the Capitol were victims of entrapment,” U.S. Sen. Dick Durbin (D-Ill.) said. “Moreover, Smith is not remotely qualified to be a U.S. Attorney. He’s going to be in the package — take it or leave it. Prior to becoming the interim U.S. Attorney, he had no courtroom or litigation experience whatsoever. None. And Smith’s lack of experience has had real-world consequences.”
Prior to his work in the Wyoming state legislature, Smith worked as Director of Planned Giving for the Family Research Council, an organization that describes homosexuality as “harmful” to society with “negative physical and psychological health effects.”
The organization also believes that sexual orientation “should [not] be included as a protected category in nondiscrimination laws or policies, as it is not comparable to inborn, immutable characteristics such as race or sex.”
During questioning before the U.S. Senate, he denied that his work with the organization shows he has loss of impartiality when it comes to matters of LGBTQ rights.
Also questioning, Smith was asked about a now-deleted Facebook post in which he appeared to express support for Kim Davis, the Kentucky county clerk who was found to be unconstitutional in her refusal to issue same-sex marriage licenses, despite Obergefell v. Hodges.
“Perhaps Hillary and Obama can share the cell with Kim Davis for refusing to uphold the Defense of Marriage Act,” the post said.
When asked why he posted it, Smith told Durbin: “I do not recall.”
Josh Sorbe, spokesperson for the Senate Judiciary Committee Democrats and Durbin, said:
“Anti-LGBTQ+ extremist Darin Smith has no business serving as a top law enforcement officer in any state — let alone a state with as much history of queer importance as Wyoming. He’s an unqualified insurrectionist with no experience litigating criminal or federal matters, and his bigotry puts into serious question his commitment to upholding the law for all Americans.”
Human Rights Campaign Vice President of Government Affairs David Stacy also condemned Smith’s confirmation to the U.S. Attorney’s office.
“The justice system in America is supposed to be about ensuring the law is applied fairly and equally. But Darin Smith has spent his career obsessed with making life worse for LGBTQ+ people, opposing marriage equality, cosponsoring state legislation targeting transgender youth, and smearing LGBTQ+ people in public statements,” Stacy said. “Just over two decades after Matthew Shepard was brutally murdered in that same state, Wyoming deserves better than tired anti-LGBTQ+ hate at the helm of federal law enforcement. The Senate should reject Darin Smith and demand a nominee who will put the people — and justice — first.”

Elevated Living. Personalized Care.

Politicians, activists pay tribute to Barney Frank

Skipping Memorial Day crowds in Rehoboth Beach

What is queer food?

GLAA’s 2026 primary election ratings show candidates agree on basics

Disillusioned about democracy? Think of it as a community garden

Honey, have we been priced out of gay paradise?

IDAHOBiT a reminder we all must stand up against transphobia

PHOTOS: Blade Summer Kickoff Party




