News
Clinton emails: ‘We should emphasize LGBT human rights’
Former secretary of state responds to Iraq, creation of LGBT liaison


Hillary Clinton called for emphasis of LGBT rights in her State Department emails. Washington Blade photo by Michael Key)
Clinton, who’s now pursing the Democratic nomination for president in 2016, expressed the view in response to a 2009 Voice of America report forwarded to her by adviser Cheryl Mills on the alleged murder and torture of gay Iraqi men, many of whom reportedly said they were more secure under the regime of Saddam Hussein.
Clinton responded 11 minutes after Mills sent her the article.
“So sad and terrible,” Clinton writes. “We should ask Chris Hill to raise this w govt. If we ever get Posner confirmed we should emphasize LGBT human rights.”
The Chris Hill to which Clinton is referring is likely the U.S. ambassador to Iraq during the first two years of the Obama administration. Posner is likely Michael Posner, who came to serve in the State Department after his confirmation as assistant secretary of state for democracy, human rights and labor.
Clinton’s call for pushing LGBT rights within the State Department is consistent with her stated philosophy that “gay rights are human rights and human rights are gay rights” and her 2011 speech in Geneva in which she highlighted international LGBT rights concerns.
Other emails in the batch unveiled on Tuesday, which span from March to December 2009, demonstrate the hang-wringing on the perceived lack of progress on LGBT issues in the first years of the Obama administration and the potential creation of a State Department official dedicated to LGBT human rights.
The emails reveal that among the individuals forwarding articles to the Clinton State Department on LGBT rights was Richard Socarides, a gay New York-based advocate who advised former President Bill Clinton on gay rights issues.
Socarides told the Washington Blade that as a former White House official he sometimes passed along information and reports he thought would be of interest to the State Department. Sometimes, Socarides said, Clinton’s staff reached out to him with a specific question.
“From what I can tell, these emails are all part of that back-and-forth,” Socarides.
In one email to Mills, Socarides forwards a Gay City News article on anti-LGBT brutality in Iraq and writes, “You guys will have to deal with this at some point if not already.”
In response to the exchange, Socarides expressed satisfaction with how issues related to the rights of LGBT Iraqis were handled, saying it was part of ongoing concern about the country and “raised by our government at many levels and on repeated occasions.”
In another email dated May, 22, 2009, Mills forwards to Clinton an article in the Advocate on a draft letter signaling the State Department’s intention to extend partner benefits to gay Foreign Service officers.
Clinton’s response isn’t revealed, but Mills commentary on the article is simply “Oh my.”
In another December 2009 email in which he forwards a Voice of America article on evangelical leaders spreading anti-gay sentiment in Africa, Socarides recommends the creation of an international LGBT point person.
“There is a lot of appreciation for everything the Dept has done around this so far and I think you could really build on it by putting someone there in charge of international LGBT human right issues,” Socarides said.
Socarides’ email was in turn forwarded to Clinton by Mills, who endorsed the idea, saying, “I think this is a good idea — what do you think?”
Clinton’s initial response was “Mira patel in sp told me she is already starting to do this. Do you want someone in drl.” The rest of Clinton’s response is redacted by the State Department. Mira Patel served at the State Department as an advisor for Clinton after having served on her Senate staff.
The response from Clinton apparently wasn’t adequate for Mills, who responded she “would want someone higher profile” and Patel is likely preparing a “response to incoming rather as an affirmative agenda.”
“Not sure how I got to be the person pushing all things in this area — think from the earlier reports on family benefits but as a general matter — we have a reaction mechanism right how (to others, to me sending emails re Uganda (and now Uganda is doing same kind of anti-gay law)) etc.,” Mills writes. “This would be someone who’s profile would be an affirmative agenda.”
Clinton has a short response to Mills eight minutes later, “Let’s discuss.” The Clinton emails don’t reveal the resolution of this discussion, which may have been taken offline.
In response to the email exchange, Socardies pointed to the appointment of Daniel Baer as deputy assistant secretary in the Bureau of Democracy, Human Rights & Labor. Part of the portfolio for Baer, who now serves as U.S. ambassador to Organization for Security & Cooperation in Europe, was international LGBT rights issues.
No specific LGBT international affairs official was appointed during Clinton’s tenure, but the State Department named Randy Berry as special envoy for the human rights of LGBTI persons under current Secretary of State John Kerry.
The emails unveiled by the State Department aren’t the last missives expected to be made public. As a result of a Freedom of Information Act request and the direction from Clinton herself, the emails are slated to keep coming on a rolling basis and all 55,000 pages should be public by Jan. 29. Clinton deleted an estimated 32,000 emails on recommendation from her legal team.
Over the course of her tenure at the State Department period, Clinton opposed same-sex marriage. The Blade could find no emails discussing the issue or any potential evolution on her views. Clinton endorsed same-sex marriage after she left the State Department in 2013.






District of Columbia
D.C. Council approves expanded grant funding for Mayor’s Office of LGBTQ Affairs
Measure introduced by Zachary Parker faces second vote

The D.C. Council on June 9 gave its first round of approval to an amendment to the city’s fiscal year 2027 budget that calls for increasing the number and size of funding grants that the Mayor’s Office of LGBTQ Affairs provides for local organizations providing services for the LGBTQ community.
The amendment, titled the “LGBTQ Community Grant Amendment Act of 2026,” was introduced by D.C. Council member Zachary Parker (D-Ward 5), the Council’s only gay member.
The amendment calls for the LGBTQ Affairs office to issue a $980,000 grant in fiscal year 2027 to a private, nonprofit organization in partnership with the office “for the purpose of supporting programs that promote the welfare of the lesbian, gay, bisexual, transgender, and questioning community.”
The organization would also initiate its own fundraising effort to expand the amount of funds beyond the amount the office would provide, enabling it to provide larger grants to a greater number of local LGBTQ organizations.
Among other things, the amendment says the organization chosen for this new role should have a “proven track record of success in grant making and fundraising” and agree to undergo an annual audit and submit quarterly reports to the office on its use of the funds it receives.
Under its rules for approving legislation, the Council must hold the second vote on the budget bill with the Parker amendment before it is sent to Mayor Muriel Bowser for her signature. It must then go to Congress for a congressional review that does not require approval, but could result in a vote to disapprove the measure, an action Congress usually does not take.
In a June 12 statement, the D.C. LGBTQ Budget Coalition called the D.C. Council’s initial approval of the Parker amendment, “a historic measure that establishes the District’s most sustainable model for a vehicle for investing in LGBTQ communities.”
The statement adds, “The legislation arrives at a critical moment, as LGBTQ-serving organizations face unprecedented uncertainty. Growing demand for services is colliding with shrinking resources, federal attacks on LGBTQ programs, and ongoing threats to local funding streams.”
It says the new program that the Parker amendment would create, if it reaches final approval, “creates a durable mechanism to protect and expand investments in the organizations that thousands of District residents rely upon every day.”
A spokesperson for the mayor’s office said he was looking into the mayor’s position on the Parker amendment but didn’t immediately get back with a response.
Germany
German group slams White House’s LGBTQ rights record ahead of World Cup
LSVD says trans, nonbinary soccer fans safety ‘not guaranteed’ in US

A German advocacy group on the eve of the 2026 World Cup sharply criticized the Trump-Vance administration over its anti-LGBTQ policies.
The World Cup will take place in the U.S., Canada, and Mexico through July 19. The tournament began on Thursday in Mexico City with Mexico beating South Africa 2-0.
“In the USA, democracy is being gradually dismantled,” said Julia Monro of Federation Queer Diversity, a German LGBTQ and intersex rights group known by the acronym LSVD, in a statement released on Wednesday. “In particular, the human rights of trans, intersex, and nonbinary individuals, as well as other queer people, are facing massive attacks and political instrumentalization by the Trump administration.”
The LSVD statement notes sports “has a special responsibility in this situation because it conveys values worldwide that extend beyond the playing field: fairness, respect, and inclusion.”
“This must apply to everyone, including trans* and nonbinary people,” says LSVD. “Those who love sport must also protect those who can only experience it under difficult circumstances.”
“The public visibility of queer people is being pushed back, companies and organizations with diversity strategies are being pressured, and laws for trans*, intersex, and nonbinary people are being tightened,” added the group. “This is not a fringe issue, but directly affects everyday life, mobility, and safety. The way minority rights are treated is a measure of the state of a democratic society. Inhumane measures must not be normalized. The international community must not remain silent as attention on the host country, the USA, increases. The Trump administration could exploit this media platform for further inhumane purposes, in order to transfer its homophobic agenda to other countries.”
LSVD also stressed the “safety of trans* and nonbinary soccer fans is currently not guaranteed in the USA.”
“We advise all queer fans to inform themselves carefully beforehand and to take precautions for their safety,” it said.
The Council for Global Equality is one of the more than 100 organizations that issued a travel advisory for the U.S. ahead of the World Cup.
LSVD in its statement pointed out the German government in 2025 issued a travel advisory for trans and nonbinary people who are planning to visit the U.S. The warning specifically noted President Donald Trump’s executive order that banned the State Department from issuing passports with “X” gender markers.
InterPride, the organization that coordinates WorldPride events, issued a travel advisory for trans and nonbinary people who planned to travel to the U.S. for WorldPride that took place last summer in D.C.
“Due to an executive order issued by the U.S. president on Jan. 20, all travelers must select either ‘male’ or ‘female’ when applying for entry or visas. The gender listed at birth will be considered valid,” read the InterPride advisory. “If your passport has ‘X’ as a gender marker or differs from your birth-assigned gender, we strongly recommend contacting the U.S. diplomatic mission before traveling to confirm entry requirements.”
LSVD notes the German government reiterated its 2025 travel advisory ahead of the World Cup.
“Anyone traveling with a different gender entry, with an ‘X’ marker in their passport, or who does not conform to the state’s expectations during checks, must expect problems in the USA,” said LSVD.
Virginia
Gay 1920s-era Hollywood star to be honored in Staunton, Va.
Billy Haines became acclaimed designer after anti-gay policies ended his acting career
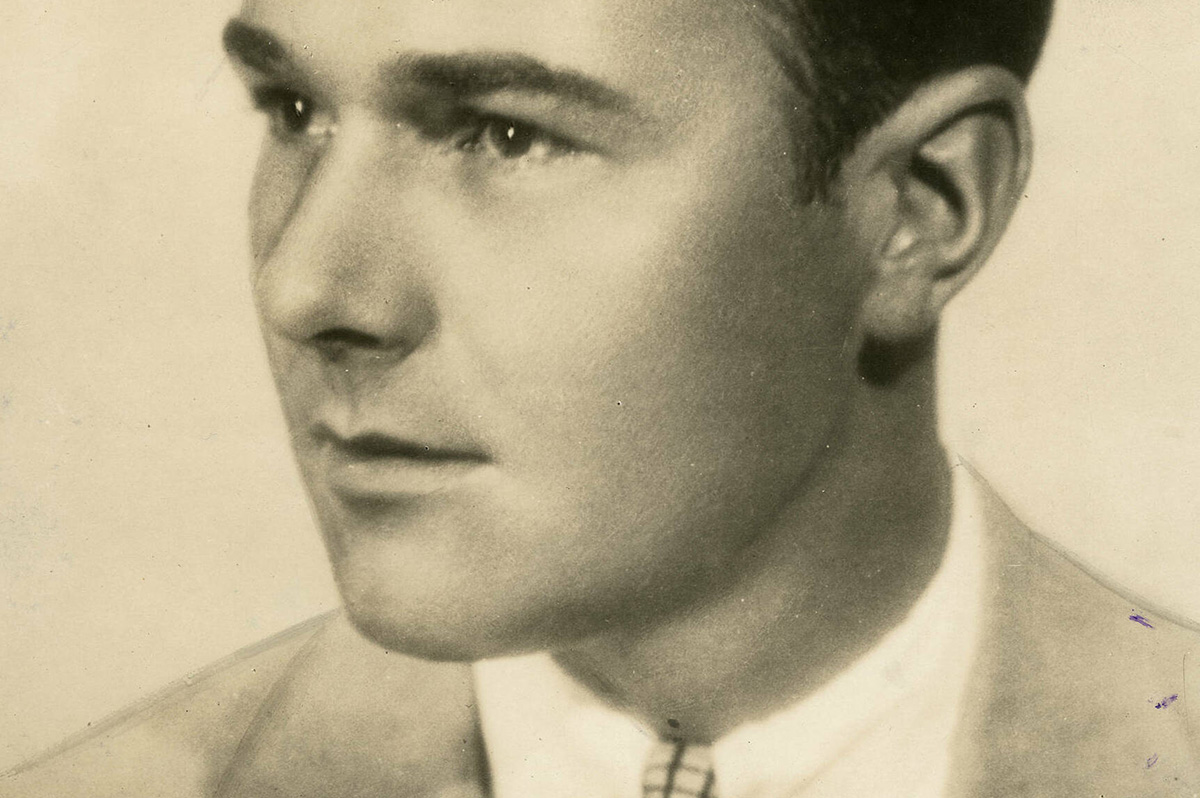
A project is underway in Staunton, Va., to honor William ‘Billy’ Haines, who was born and raised in Staunton before becoming an out gay 1920s and early 1930s-era Hollywood movie star whose acting career ended around 1934 when he refused demands that he conceal his sexual orientation and end his relationship with his male partner.
Haines left the movie business around that time to start what became a highly successful interior design and furniture business in Los Angeles that he led until his death in 1972 at age 72, and which remains in business today, according to the Arcadia Project, a Staunton-based nonprofit initiative.
In a statement released last month, Arcadia Project announced it is working to revitalize a long-vacant movie theater in downtown Staunton that it plans to rename after Haines. It says a fundraising campaign is under way to support efforts to reopen the theater and the larger building in which it is housed as a “dynamic mixed-use cultural center.”
The statement notes that Haines left Staunton at age 14 and resided in Hopewell, Va., and Greenwich Village in New York City until 1922, when he was “discovered” by a talent scout and sent to Hollywood.
“Between 1922 and 1934, Haines appeared in 54 movies during his meteoric and highly successful career,” the Arcadia Project statement continues, noting he transitioned from silent movies to talkies and was fully open about being gay. “But when Hollywood’s moral crackdown of the 1930s demanded that he end his relationship with his longtime partner Jimmie Shields, Haines refused,” it says.
“For LGBTQ people – then and now – Haines’s choice resonates deeply. Rather than deny who he was, he reinvented himself as an interior designer to the stars,” according to the statement.
It says he helped invent the so-called Hollywood Regency style home and designed homes for Hollywood legends such as Joan Crawford, Gloria Swanson, Carole Lombard, George Cukor, and Jack Warner as well as for political figures like Ronald Reagan when he was governor of California.
“As there is no monument, marker or public recognition for Haines in his hometown of Staunton, Va., Arcadia Project, in collaboration with the LGBTQ+ community in Staunton seeks to commemorate him inside a new cultural center,” the statement says.
It quotes Arcadia Project Executive Director Pamela Mason Wagner as saying, “Naming the movie theater in Haines’ honor is more than an act of historical recognition – it is a powerful statement about visibility, belonging, and whose stories are valued in our community.”
The statement says project leaders hope to open the cultural center in early 2027, with a fundraising campaign seeking to raise $250,000 to renovate the theater.
“If the full goal is not reached, a smaller space within the building will be named for Haines, scaled to the amount of funds raised,” it says. “We truly hope friends and admirers of Billy Haines everywhere will want to participate.”
Donations for the project can be made through this site: www.thearcadiaproject.org

PHOTOS: The Audacity Brunch

D.C. Council approves expanded grant funding for Mayor’s Office of LGBTQ Affairs

Congressional Cemetery hosts Gays & Graves

Baltimore Pride is here

Calendar: June 12-18

Hundreds of thousands expected to attend D.C. Pride events

PHOTOS: Pride Run

Queen Jean is Tony’s first transgender winner

David Archuleta, Monroe Alise named D.C. Pride parade marshals




